To get the data I'll be presenting below, first I excluded participants who stated on the survey that they did not adhere to the diet. Next, I excluded participants who were gluten-free before January, because they would presumably not have experienced a change from continuing to avoid gluten. That left us with 53 participants.
For each of these graphs, the vertical axis represents the number of participants in each category. They won't necessarily add up to 53, for several reasons. The most common reason is that for the questions asking about changes in health conditions, I didn't include responses from people who didn't have the condition in question at baseline because there was nothing to change.
Question #1: What is your overall opinion of the effect of gluten free January on you?
 Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.
Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.Question #2: Did you note a weight change at the end of gluten free January?
 And here are the data for people who described themselves as overweight at baseline:
And here are the data for people who described themselves as overweight at baseline: Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.
Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.Question #3: Before January 2011, did you have a problem with intestinal transit (frequent constipation or diarrhea)? If so, did your symptoms change during the month of January?
Responses are heavily weighted toward improvement, although there were a few instances where transit worsened. Transit problems are one of the most common manifestations of gluten sensitivity.
Question #4: Before January 2011, did you have frequent digestive discomfort (pain, bloating, etc.)? If so, did your symptoms change during the month of January?

Digestive discomfort was common, and the gluten-free diet improved it in nearly everyone who had it at baseline. I find this really impressive.
Question #5: Before January 2011, did you have acid reflux? If so, did your symptoms change during the month of January?
 Acid reflux responded well to a gluten-free diet.
Acid reflux responded well to a gluten-free diet.Question #6: Before January 2011, did you have a problem with tiredness/lethargy? If so, did your symptoms change during the month of January?
 Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.
Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.Question #7: Before January 2011, did you have a problem with anxiety? If so, did your symptoms change during the month of January?
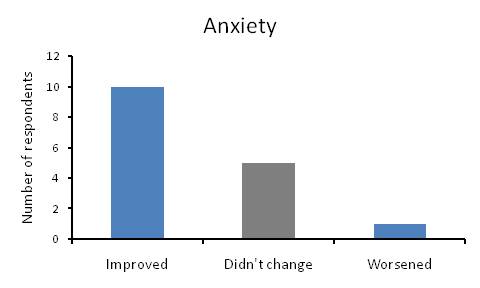 Anxiety tended to improve in most participants who started with it.
Anxiety tended to improve in most participants who started with it.Question #8: Before January 2011, did you have a problem with an autoimmune or inflammatory condition? If so, did your symptoms change during the month of January?
 Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms.
Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms. Question #9: If you ate gluten again or did a gluten challenge after gluten free January, what was the effect?
 Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.
Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.Conclusion
I find these results striking. Participants overwhelmingly improved in every health category we measured. Although the data may have been somewhat biased due to the 53% response rate, it's indisputable that a large number of participants, probably the majority, benefited from avoiding gluten for a month. At some point, we're going to compile some of the comments people left in the survey, which were overwhelmingly positive. Here's a typical comment in response to the question " In your own words, how would you describe your January 2011 experience" (used with permission):
Amazing! I would recommend the experiment to anyone. I felt completely more alert, and less bloated. When I ate some gluten at the close of the experiment, I felt gross, bloated, and lethargic.I think it's worth mentioning that some participants also eliminated other starches, particularly refined starches. Judging by the comments, the diet was probably lower in carbohydrate for a number of participants. We may try to assess that next year.




